Japanese group to take induced pluripotent stem (iPS) cell-derived retinal cells into the clinic

Stem cells. Source: http://bit.ly/ZnYuFS
As reported in Nature News on 27 February 2013 ophthalmologist Masayo Takahashi M.D., Ph.D. and her colleagues at the RIKEN Center for Developmental Biology (Kobe, Japan), plan to submit an application to the Japanese health ministry for a clinical study of induced pluripotent stem cell (iPS)-derived cells. The researchers planned to submit their application in March 2013; if approved, they could begin recruiting patients as early as September.
The author of the Nature News article is Nature‘s Asian-Pacific Correspondent, David Cyranoski, who is based in Tokyo.
The researchers plan to treat approximately six people with severe age-related macular degeneration (AMD). Specifically, the researchers are targeting “wet” AMD, in which angiogenic blood vessels invade the retina, destroying the retinal pigment epithelium (RPE) that supports the light-sensitive photoreceptors.
AMD is a common cause of blindness that affects at least 1% of adults over 50. Wet AMD can be treated with anti-vascular endothelial growth factor (anti-VEGF) agents such as ranibizumab (Genentech/Novartis’ Lucentis), pegaptanib (Gilead/OSI/Pfizer’s Macugen), aflibercept (Sanofi/Regeneron’s Eylea), and–off-label–small doses of the anticancer agent bevacizumab (Genentech/Roche’s Avastin). However, the use of these agents requires that they be injected repeatedly into the eye.
According to the Nature News article, Dr. Takahashi and her colleagues will take an upper arm skin sample the size of a peppercorn, and transform the cells from this sample into iPS cells by using specific proteins. They will then add other factors that will induce differentiation of the iPS cells into retinal cells. Then a small sheet of these retinal cells will be placed under the damaged area of the retina, where they are expected to grow and repair the damaged RPE.
Although the researchers would like to demonstrate efficacy of this treatment in ameliorating the disease, the main focus of these studies will be on safety. Safety concerns include immunogenicity of the transplanted cells, and formation of tumors if the transplanted cells multiply uncontrollably. Another concern is that the transplanted cells might fail to engraft, and to integrate with the host tissue. It is also possible that the RPE identity of the transplanted and differentiated cells might not be stable over time.
With respect to these concerns, studies published by Japanese researchers in 2013 (Araki et al.) and reviewed in a recent Nature News article contradicted the original mouse studies that suggested that syngeneic or autologous iPS cells might be immunogenic.
With respect to tumor formation, Dr. Takahashi’s proposed studies will involve using only a few iPS cells, thus reducing the probability of forming tumors. Moreover, since the eye is relatively accessible, any tumors would be relatively easy to remove.
In addition, Dr, Takahashi has presented preclinical studies at conferences, which indicate that her iPS cells do not form tumors in mice and are safe in non-human primates. (Dr. Takahashi’s preclinical studies have also been submitted for publication.) The studies have provided reassurance of the cells’ safety to at least some leading researchers, such as Martin Pera (University of Melbourne, Australia) and George Daley (Harvard Medical School, Boston MA).
However, other researchers believe that to take iPS cell-derived tissue into the clinic at this time is premature. Robert Lanza, M.D., the chief scientific officer at Advanced Cell Technology (ACT) (Santa Monica CA) says that he cannot imagine regulatory agencies permitting studies such as Dr. Takahashi’s without years of preclinical testing.
As mentioned in the Nature News article, ACT has a program involving human embryonic stem cell (hES cell) and iPS-derived platelets for transfusion. This program is in the preclinical stage. Since platelets lack a nucleus and cannot form tumors, it is inherently less risky that clinical programs of stem-cell (and especially iPS cell) derived differentiated cells that have nuclei.
Dr. Takahashi’s proposed study of her therapy in humans is considered a “clinical study”, not a clinical trial. In Japan’s regulatory system, clinical studies are less tightly regulated than clinical trials. However, a clinical study cannot by itself lead to approval of a potential therapeutic for clinical use as a treatment. If Dr. Takahashi’s clinical study data is positive, that might attract investors or help her to get approval for a formal clinical trial. As in the U.S. or Europe, successful clinical trials will be required if Dr. Takahashi’s cellular therapy is ever to be used to treat patients.
Dr. Takahashi’s clinical study was approved by institutional review boards at both the natural sciences institute RIKEN in Wako and the Institute of Biomedical Research and Innovation in Kobe, where the surgical procedures will be carried out. Final approval will depend on the action of a committee of the Japanese Ministry of Health, Labour and Welfare. If Dr. Takahashi wins approval by September 2013 as expected, it will take another eight months to produce the tissue implants needed for her clinical study.
Other retinal repair programs involving human embryonic stem cell-derived RPE cells
Dr. Takahashi’s research does not represent the only RPE cell-based retinal repair program now being developed. There are at least two others, both of which are based on hES cells, not iPS cells.
As was not mentioned in the Nature News article, ACT has Phase 1 trials underway in its own RPE retinal repair program. ACT’s RPE cells are derived from human embryonic stem cells (hES cells). The company’s Phase 1 safety studies are in Stargardt’s Macular Dystrophy (SMD) and in dry AMD (which results from atrophy of the RPE layer, and causes vision loss through loss of photoreceptors in the central part of the eye. Dry AMD does not involve angiogenesis.). SMG is a rare inherited juvenile macular degeneration.
In February 2012, Dr. Lanza and his academic collaborators at the University of California at Los Angeles published a preliminary report of their clinical studies in dry AMD and SMG. In this study, one patient with each of the two conditions was treated with hES cell-derived RPE cells. The hES cell-derived RPE cells showed no signs of hyperproliferation, tumorigenicity, ectopic tissue formation, or apparent rejection after 4 months. Neither patient showed loss of vision, and there were signs of improvement of vision. As a result of this very preliminary study, the researchers decided in the design of future clinical studies to treat patients earlier in the disease processes, potentially increasing the likelihood of improvement of vision.
The other RPE-based retinal repair program is a collaborative effort between Neusentis (A Cambridge U.K. and Durham NC-based Pfizer research unit) and “The London Project” which was formed by Professor Pete Coffey [Institute of Ophthalmology, University College London (UCL)] and his collaborator Lyndon da Cruz (Moorfields Eye Hospital) to develop cellular therapies for all types of AMD. The London Project began collaborating with Pfizer in 2008; this collaboration was brought under the aegis of Neusentis when it was formed in 2011. Research is based on RPE cells derived from hES cells.
The Neusentis/London Project group claims to have developed a deep understanding of the biology of hEC cell-derived RPE cells, and to have worked out methods of producing enough RPE cells under GMP conditions to support clinical studies. They also claim to have developed a clear approach to establishing the safety of the therapy via preclinical studies. The collaborative group is now moving towards clinical studies of their therapies, which they “hope to achieve in the not too distant future”.
As we discussed in our February 15, 2011 article on this blog, Pfizer–as of February 1, 2011–closed its Memorial Drive laboratory in Cambridge, MA. This laboratory housed most of Pfizer’s regenerative medicine research, as well as the company’s RNAi therapeutics research group. However, as we said in this article, Pfizer was folding its Cambridge, UK regenerative medicine group–“which had been focusing on development of preclinical embryonic stem (ES) cell-based ophthalmology therapies, in collaboration with the University of London”–into a “new pain and sensory disorder research unit”. According to its website, Neusentis, which was formed in 2011, has “a particular focus on pain and sensory disorders”.
Japanese government backing for iPS cell research and commercialization
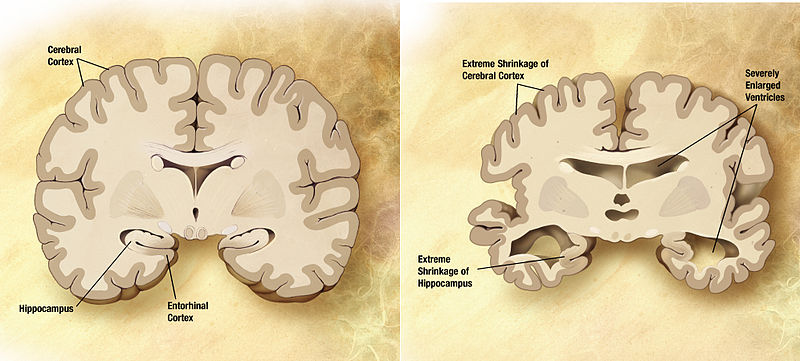
Japan has been a hotbed of iPS cell research, since these cells were first produced by Shinya Yamanaka, M.D. Ph.D. (Kyoto University) in 2006. He received The Nobel Prize in Physiology or Medicine in 2012 for his work on iPS cells. The co-recipient of the Prize, Sir John B. Gurdon, successfully cloned a frog using intact nuclei from the somatic cells of a Xenopus tadpole back in 1958. The two scientists received the 2012 Prize “for the discovery that mature cells can be reprogrammed to become pluripotent”. Since their discovery, iPS cells have been employed in such areas as basic research, disease modeling, and drug screening. (Follow this link for a recently-published example of the potential use of iPS cells in designing personalized treatments for Alzheimer’s disease.)
In 2013, as part of its stimulus package, the Japanese government has been providing generous funding for iPS research. This funding includes ¥700 million for a cell-processing centre at the Foundation for Biomedical Research and Innovation in Kobe, mainly to support Dr. Takahashi’s regenerative medicine research. In general, the iPS funding under the stimulus is aimed at moving university research on iPS cells into commercial and medical applications.
Moreover, according to Mr. Cyranoski’s 27 February 2013 Nature News article, the Japanese parliament is expected to rule by late June 2013 on a provision of a revised drug law, which would fast-track iPS-based therapies that appear to be effective in phase 2 or phase 3 trials. However, the success of the Japanese government’s efforts to accelerate commercialization of iPS-based therapies may depend in part on the success of Dr. Takahashi’s clinical research.
________________________________
As the producers of this blog, and as consultants to the biotechnology and pharmaceutical industry, Haberman Associates would like to hear from you. If you are in a biotech or pharmaceutical company, and would like a 15-20-minute, no-obligation telephone discussion of issues raised by this or other blog articles, or an initial one-to-one consultation on an issue that is key to your company’s success, please contact us by phone or e-mail. We also welcome your comments on this or any other article on this blog.